
CASE STUDY 6
![]() SECTOR: NHS
SECTOR: NHS
DELIVERABLE: New Multifunction Service Desk
THE CLIENT: The Queen Elizabeth Hospital King’s Lynn NHS Foundation Trust
The Queen Elizabeth Hospital King’s Lynn NHS Foundation Trust (QEH) is a 514 bed general hospital providing services to approximately 220,000 people in West Norfolk, North East Cambridgeshire and South Lincolnshire. It is also the largest regional employer employing approximately 2400 staff.
All NHS hospitals have been targeted by the UK government to make financial savings over a 5 year period. These targets are significant and therefore require transformational change in the way the many hospitals operate, their productivity and efficiency levels and the services they deliver, i.e. major changes are required to their existing configuration of people, processes and technology. QEH has started on this journey.
At the beginning of their organisational review QEH had identified that they had at least 9 separate internal help desks offering support (with different / poor standards of customer service) to the same body of staff. Despite the hospital being a 24/7 service, help desk hours were limited to normal business hours. The hospital believed that potential productivity and efficiency savings could be achieved by consolidating the 9 help desks into a single service desk.
EBME = Electro-biomedical Engineering
? =Support teams / help desks yet to be identified
QEH’s key business objectives for implementing this change initiative were:
• to reduce costs through 1) the consolidation of a number of help desks, 2) using technology to facilitate self-service and 3) multiskilling fewer service desk agents
• to improve service levels and internal controls through implementing best practice and standardised business processes and reporting, thereby leading to improved staff productivity through quicker issue / query resolution
• to improve the overall customer experience by implementing a single contact point and a unified experience irrespective of query
• to create revenue generating opportunities for the Trust by building a scalable service on a common voice and data platform that could be used to insource work from other businesses (blue cloud in previous diagram)
Two previous project managers had tried to get this project up and running but had failed to progress it further than submitting a business case.
For a number of years there had also been a significant underinvestment in QEH’s core voice and data network. Another project had therefore been set up to address this and complete a total refresh of its wired and wireless voice and data network within 2 years. This project and its extended timescale was likely to have an impact on delivering the Service Desk Project
Zebrazoo Consulting was appointed to turn the Service Desk Project around and implement a solution that could deliver the stated project objectives.
Key Areas of Change:
• Business process re-engineering
• Workforce optimisation
• Organisational redesign
• Technology change
• Customer service improvement
• Culture change
Zebrazoo Consulting’s Impact:
Our review of the existing business case identified the following key issues:
• There was no clear service desk model being applied
• No feasibility study had been undertaken to identify whether any of the 9 proposed help desks would fit with the concept of a consolidated service desk and, if so, would actually generate any benefits
• As no feasibility study had been undertaken there had also been no communication or marketing of the vision of a single service desk with key stakeholders from the 9 existing helpdesks
• The project budget had been significantly understated. No provision had been made for any implementation or project management costs
• The funding allocated to purchase new service desk software had to be spent by the (imminent) financial year end and could not be carried over into the next year.
Zebrazoo Consulting therefore put the following plan in place:
• A clear end state multi-channel service desk model was proposed as per the diagram below. Once signed off by the project’s executive steering committee this would become the foundation which the project plan could be structured
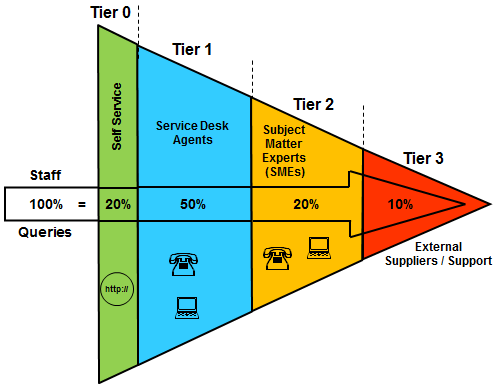
• Tier 1 service desk agents would be multi skilled. They would have a primary core skill e.g. IT (first line fix) and be trained with a secondary and possibly tertiary skill e.g. the skills to support Smartcards and Hospital Information Systems (HIS). This, in conjunction with the use of Tier 0 self service, would mean fewer agents would be required to support the current help desks’ workload
• A single service desk telephone number would exist and an ACD / IVR Telephony solution would be used to route calls in the first instance to an agent with the correct primary skillset but, if they were all busy, skills based routing would route the caller to an available agent who had the appropriate secondary or tertiary skillset to log / resolve the customer’s query
• New off the shelf / market leading service desk software would be purchased to underpin the new service desk, or if this did not go ahead, underpin the IT help desk (the largest help desk) that was currently using software that was not fit for purpose
• A communication and training programme would be put in place to encourage staff to use self service in the first instance wherever possible
• Switchboard, which already operated a 24hr service, would be multi skilled to enable their staff to log and escalate queries that arose outside of standard business hours. Service Desk and Switchboard would be brought together under one manager
• A detailed communication and marketing plan would be drafted and project kick off meetings scheduled as soon as possible with all key stakeholders
• As soon as the kick off meetings had taken place a retrospective feasibility study would be started for each existing help desk. This would include:
- Documenting their ‘as is’ business processes and reviewing the suitability for migrating/standardising these into a consolidated service desk
- Documenting business volume indicators by process
- Documenting any existing service levels with the business
- Completing a ‘people versus process’ matrix to determine what proportion of a person’s role was allocated to actual help desk processes and what proportion was allocated to other non-helpdesk business activity
• Interdependencies with other projects would be clearly understood and used to shape the final scope and timeframe of the project
• An appropriate location for the new Service Desk would need be identified and appropriately refurbished to emphasise a break from the existing help desk culture
• A new budget would be submitted for approval.
The Feasibility Study
Analysis from our retrospective feasibility study indicated:
• With the exception of Estates, Hotel Services and Switchboard it would be feasible to move all or some of the helpdesk activity to a new service desk.
• Switchboard would be viable to support the service desk out of hours
• Of those help desks suitable for consolidation only IT, Smartcards, and Portering had staff who were almost exclusively engaged in helpdesk activity. The remaining help desks had staff that split their roles fairly evenly between help desk activity and other business activity
• Due to the activity split of the staff working on some of the helpdesks, actual headcount savings to the QEH would be minimal as roles would still need to remain in the organisation to undertake the non-helpdesk activity
• The migration of Portering and the Medical Equipment Library (MEL) to the new service desk was dependent on the network refresh project delivering a hospital wide wireless network to enable porters to use handheld devices and MEL to benefit from being able to locate radio frequency identification (RFID) tagged equipment
• Analysis of the existing IT help desk highlighted that while it was the largest help desk in the hospital in terms of annual call volumes there were significant staff performance and behavioural issues.
• A hospital wide online survey of the performance of the existing service desks indicated that ‘customer service’ was almost non existent
• There was no on-going funding available to recruit an external person into the Head of Service Desk role to help change the culture and revolutionise the service. The role would have to be filled by an existing help desk manager
• As no other hospital space was available, the space occupied by the IT helpdesk would need to be redesigned and refurbished to accommodate a consolidated service desk
• Other than for the IT helpdesk there were a) no SLA’s between the existing help desks and the business and b) management information on help desk / agent performance was almost non existent
Based on the results of the feasibility study Zebrazoo Consulting made the following recommendation to the Executive Steering Committee:
• Despite there being limited headcount savings available a new consolidated service desk should still be pursued as this would generate significant productivity savings and would create a scalable solution should the Hospital wish to offer a future cloud based service
• New software had to be purchased as, irrespective of the migration, the IT helpdesk was operating on a platform that was not fit for purpose
• The migration of the various helpdesks should be phased with:
- IT and Smartcards in Phase 1
- Tier 0 Self Service, HIS and EBME in Phase 2
- Portering and MEL in Phase 3 (which would be delayed due to dependencies on the Trust’s network refresh project)
- Switchboard being trained to support the Service Desk out of hours in a final Phase 4
• All 1st line service desk roles should be made permanent. This would allow poor performing contract staff to be weeded out
• All 1st line and 2nd line service desk staff would need to put through thorough customer service training as well as the appropriate process, system and technical training (including ITIL training for IT support staff)
• The internally appointed Head of Service Desk would need mentoring and be subject to regular performance reviews
Zebrazoo Consulting’s proposals were adopted by the steering committee. An incremental budget was approved and the scope of the project was locked down.
The Delivery Phase
Working with the hospital’s procurement team an invitation to tender for the new software was held via the Buying Solutions Framework. After careful evaluation Hornbill Support Works was selected as the preferred software
All Phase 1 migrating business processes were reengineered to align with Hornbill’s best practice service desk processes
The Hornbill Support Works software was installed and configured to work with the Trust’s email server and interface with Active Directory (AD) to populate its master data database. All call profiles, hierarchies, escalation routes, call scripts, templates and initial service levels were input into the system
Staff were recruited / appointed into the new Service Desk roles and a Head of Service Desk was appointed
The new Service Desk Agents were trained to be multi skilled in handling both IT and Smartcard queries
All Tier 1 and Tier 2 staff were trained on the new processes, how to use the new software and were put through comprehensive customer service training
The new service desk environment was refurbished and electronic wallboards were installed to display real time performance data from a) the telephony switch (e.g. dropped calls) and b) the Hornbill Support Works application (e.g. open calls about to breach their SLA)
SLA’s were agreed between the Phase 1 Service Desk and the business and, where necessary, the Hornbill application was updated accordingly
The data held in AD was cleansed for go live and a separate project initiated to install a permanent link to automatically update AD with any changes to records held on the Trust / national Electronic Staff Record system
All communication with key stakeholders and the wider Trust was executed in line with the project’s Communication & Marketing plan
Phase 1 of the project went live on time and within the revised budget 8 months from when Zebrazoo Consulting was brought on board to turnaround the project.
For a printable PDF version of this case study please click here: Case Study – 6